This video was published on 2017-05-18 05:34:39 GMT by @MedLecturesMadeEasy on Youtube.
MedLecturesMadeEasy has total 87.4K subscribers on
Youtube and has a total of 794 video.This video has received 1K
Likes which are higher than the average likes that MedLecturesMadeEasy gets . @MedLecturesMadeEasy receives an average views of 24.7K
per video on Youtube.This video has received 17
comments which are higher than the average comments that MedLecturesMadeEasy gets .
Overall the views for this video was lower than the average for the profile.














































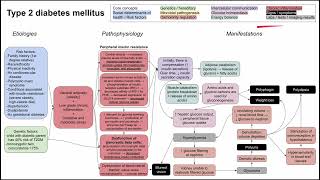



MedLecturesMadeEasy's video: Prenatal screening fetal testing and other tests during pregnancy
1K
17